Covid 19 has affected the world’s population regardless of race, gender, age, and geographical locations. At present the disease has affected over 251 million people worldwide causing over 5 million deaths. In Africa, more than 8 million people were infected by the virus causing more than 220 thousand deaths[1]. Several studies have shown that the COVID-19 pandemic has led to significant disruptions in economic activities with devastating effects on livelihoods in Africa.[2] The prospect of losing jobs, income, and fear of contracting the virus would certainly elevate the level of anxiety, depression, and stress creating serious psychosocial problem[3]. Also, the anxiety surrounding the pandemic could trigger stigma against the sick and some incidence of violence caused by the mobility lock downs.
This brief presents evidence based on high frequency data on the impact the COVID-19 pandemic had on emotional and psychosocial well being in Kenya mainly during the period March 2020-October 2020. Table 1 suggests that at the height of the pandemic (May 2020) when most governments in Africa declared lock downs and state of emergency, the percentage of households that suffered from elevated anxiety reached to 75%. As people begun to get better information on the spread of the virus, anxiety levels seem to have decreased. Still the proportion of the population suffering from serious anxiety during the pandemic exceeded 50%. A major factor driving heightened anxiety seems to be the fear of contracting the virus. Throughout the period under study, the proportion of households who felt anxious of contracting the virus hovered around 80% with no change in the trend. It is clear also from the table that while economic activity declined following the lock downs around May/July 2020, the fear of losing jobs loomed large in 2021 suggesting the gradual erosion of livelihoods in the wake of the pandemic and lack of job security and social protection.
Table 1. Incidence of Anxiety and emotional stress in Kenya: 2020/2021
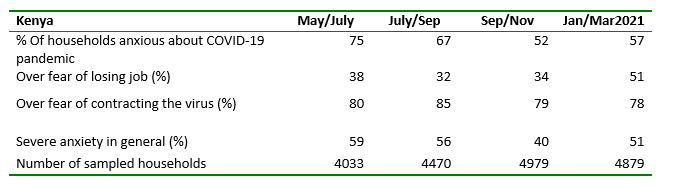
Source: authors’ computations.
- Table 1 described the trend in the degree of anxiety and mental distress in the general population. It may also be interesting to know who suffered most during this period and what important factors seem to be correlated with anxiety levels in the population?
- Table 2 suggests that anxiety levels seem to be much higher among women indicating the disproportionate burden falling on women during such shocks, in terms of taking care of the family as well as fighting the disease. According to table 2, on the average, women tended to exhibit 10% higher anxiety levels than men.
- The other important factor associated with anxiety levels is age where younger household heads exhibited relatively higher levels of anxiety compared with older ones.
- The other revealing factor associated with anxiety levels is the perceptions households have towards their government. Households that had no trust at all on government or feel indifferent about its trustworthiness suffered a significantly higher anxiety levels (52% and 72%, respectively) than those who tended to trust the government.
- This is suggestive of the underlying causes of anxiety resting on the perceived information gap as well as mistrust on the information shared by government authorities about the pandemic.
Table 2. Marginal effects from a probit model regression for Kenyan household survey.
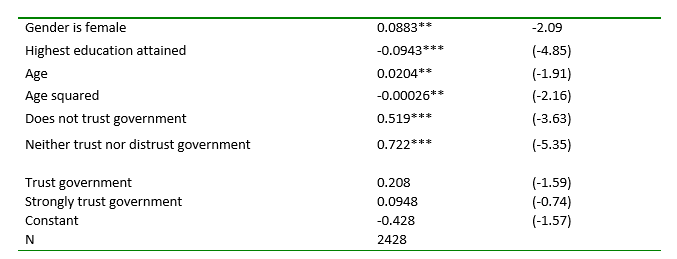
Source: authors’ computations. Note: Z statistics in parentheses * p<0.05, ** p<0.01, *** p<0.001
Related to anxiety, the pandemic such as this created the conditions for stereotyping, discriminations and stigma towards others perceived to be contracting the disease. During the pandemic, stigma is described as the one virus that is spreading even faster than the COVID-19 Pandemic[i]. The disease is new with very little-known information causing fear, panic, and misinformation. The fear of disclosing having the virus to others has brought a sense of shame in the society and created stigmatization. For fear of being stigmatized or marginalized, people tend not to disclose their status about the virus even to close family members by failing to get tested. The shame associated with disclosing of having the virus has led to substantial psychological distress, which doesn’t end there but the person infected with the virus continues transmitting the disease knowingly to the community without being tested. This cycle of fear of being infected by the virus, associated with the shame and stigmatization, coupled with economic and social uncertainties has led to a high level of mental distress among communities.
Table 3 below reports that women tend to be less stigmatizing than men (by nearly 8%) and generally the level of stigma started to decline as the virus continued to affect a large percentage of the population.
Table 3. Probit model regression on factors correlated with negative perceptions of people with COVID-19
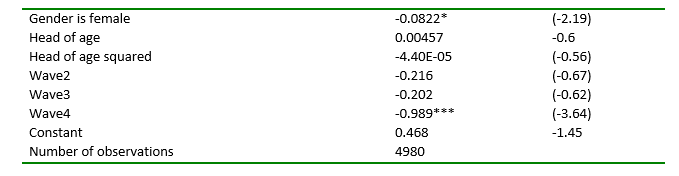
Source: authors’ computations. Note: Z-statistics in parentheses * p<0.05, ** p<0.01, *** p<0.001
Finally, the measures taken by authorities to stem the spread of the virus such as stay-at home orders, school-closing policy, public-gathering restrictions, cancellation of public events has led to enormous psychological distress and uncertainties for many people. It has also created opportunities for heightened violence such as domestic violence, gender violence, spouse violence, sibling’s violence. Table 4 reports that areas under severe lockdown had 26% higher rates of violence in Kenya suggesting the strong association between lockdowns and violence.
Table 4. Incidents of lockdown related violence

Source: authors’ computations. Note: Z statistics in parentheses * p<0.05, ** p<0.01, *** p<0.00
In conclusion, mental health problems got worse as a direct consequence of the COVID 19, and because of job losses and loss of economic opportunities. While loss of jobs tends to be temporary, some jobs may not be back. There is need to empower those that have lost jobs so that they manage the transition in these difficult times. Unfortunately, most interventions to fight the pandemic do not include mental health care despite growing evidence on the people suffering from anxiety, depression, stigma, and violence. Grassroots institutions including schools, universities, and media houses should be empowered to offer mental health care to reach the general population. Lessons should be taken on long term impact on mental health and stigma from past pandemics like HIV /AIDS and Ebola.
[1] . (https://www.worldometers.info/coronavirus/#countries, Nov 2021).
[2] Josephson, A., Kilic, T. & Michler, J.D. Socioeconomic impacts of COVID-19 in low-income countries. Nat Hum Behav 5, 557–565 (2021). https://doi.org/10.1038/s41562-021-01096-7
[3] Pfefferbaum et al (2020)https://www.nejm.org/doi/full/10.1056/nejmp2008017
[i] (Kim Robin van Daalen, 2021)